Ratification Date: 14/03/2024
Next Review Date: 30/06/2026
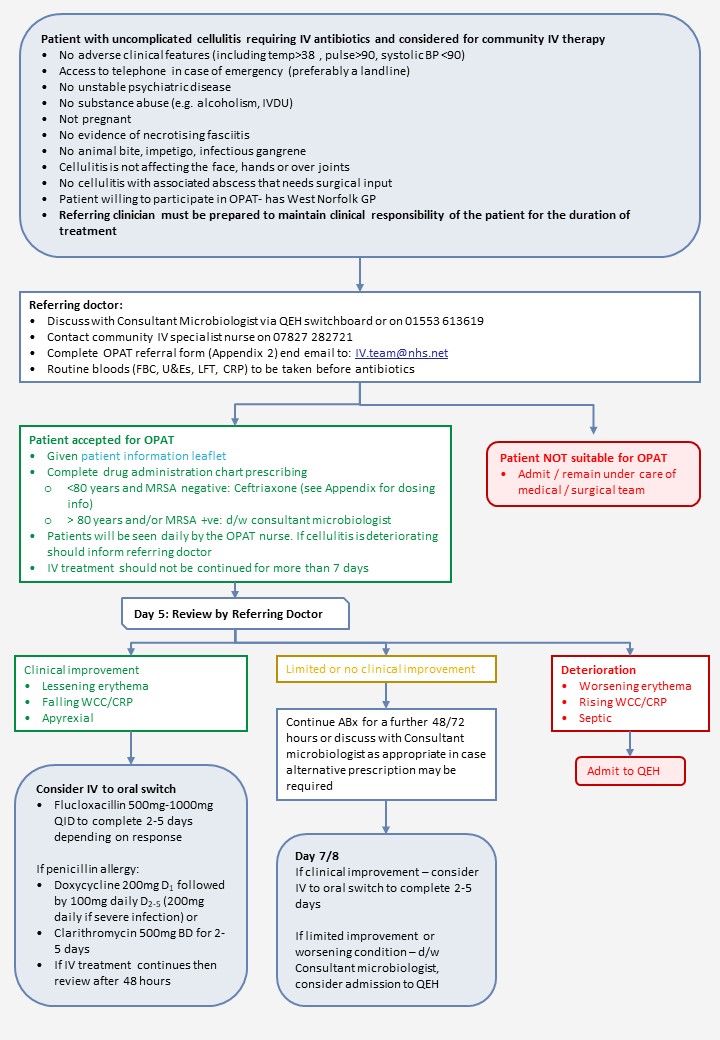
Cellulitis IV Pathway (QEH)
Cellulitis treatment notes
OPAT is for the treatment of uncomplicated cellulitis. It is not intended for the treatment of infection originating from an animal bite, impetigo, infectious gangrene or necrotising fasciitis.
Cellulitis is an acute spreading infection of the skin, which may involve the subcutaneous tissues. The area of cellulitis will be painful, swollen, erythematous and is frequently unilateral. It may follow an abrasion, insect bite or other minor trauma or tinea pedis. The most common pathogens are streptococcus spp (especially S. pyogenes and other b-haemolytic streptococci) and Staphylococcus aureus including MRSA.
In some cases, broader spectrum antibiotic cover may be required (eg for patients with diabetes). These agents may be considered ONLY after discussion with the Consultant Microbiologist.
Cellulitis may result in severe damage to the tissues, including the lymphatic system. This can take several weeks to recover and, in many cases, leads to permanent lymphatic damage and subsequent lymphoedema. Continuing antibiotics for more than a few days does not shorten this recovery period.
Cellulitis is frequently recurrent.
The diagnosis of cellulitis of the lower limb should be differentiated from:
- Deep-vein thrombosis
- Acute venous eczema
- Features of chronic lymphoedema
- Abscess
- Localised bullous pemphigoid
- Vasculitis
- Osteomyelitis
For all patients, presenting to the acute medical unit an initial assessment should be made to determine whether a patient is suitable for outpatient therapy. Particular attention should be paid to:
- Severity of infection, local and systemic features
- Presence of co-existing disease or immunosuppression
- Whether cellulitis has progressed despite adequate doses of appropriate oral antibiotics in the community
- See Erons’ cellulitis severity classification below
| Class I | Patients have no signs of systemic toxicity, have no uncontrolled co-morbidities and can usually be managed with oral antimicrobials on an outpatient basis. | Suitable for oral therapy |
| Class II | Patients are either systemically ill but no adverse clinical features (including temp>38*C, pulse>90, systolic BP <90) or systemically well but with a co-morbidity such as peripheral vascular disease, chronic venous insufficiently or morbid obesity which may complicate or delay resolution of their infection. | Suitable for OPAT |
| Class III | Patients may have a significant systemic upset such as acute confusion, tachycardia, tachypnoea, hypotension or may have unstable co-morbidities that may interfere with a response to therapy or have a limb threatening infection due to vascular compromise. | Requires in-patient treatment |
| Class IV | Patients have sepsis syndrome or severe life threatening infections such as necrotizing fasciitis. | Requires in-patient treatment |